
The institutional knowledge of a senior attending — available on every shift, every patient, every provider.
A hospitalist managing 18 patients at 2am can't hold every guideline at once. A resident without attending backup makes consequential calls alone. A locum entering an unfamiliar system flies blind. Pogosh closes the gap between what physicians know and what they can reliably access under pressure.
Pogosh is an API-first clinical decision support engine. At the point of care it surfaces the highest-yield labs to order, imaging to consider, escalation criteria to watch for, and the right specialist to call — embedded in your EMR or accessible via REST API.
Built and used daily by Pouyan Golshani, MD — practicing interventional radiologist · StatPearls IR Editorial Board · FDA AI-device research on medRxiv
Where clinical knowledge breaks down
Physicians don't miss diagnoses or over-test from lack of knowledge. They miss them from the impossible cognitive load of synthesizing hundreds of guidelines under time pressure.
The 2am hospitalist
Eighteen patients. New admit with chest pain. Old admit with sepsis trending wrong. Discharge orders waiting. The senior attending's instincts exist — but not at this hour, not for this patient, not on this provider.
The resident without backup
Consequential calls made alone. The right escalation criteria are written down somewhere — usually a PDF or a folder of departmental SOPs that nobody navigates mid-call. Knowledge exists; access doesn't.
The locum on day one
Unfamiliar system, unfamiliar protocols, unfamiliar specialists. The locum is technically excellent and operationally blind. The patients don't know the difference until something gets missed.
What Pogosh surfaces at the point of care
Open the chart. Pogosh returns four things, structured and traceable to a guideline:
What to order — and what's missing
For the working diagnosis, the labs and tests with the most diagnostic and triage yield. Compares against what's already ordered and flags gaps. No protocol-stuffing — just the labs that change management.
Try in your workflow →Which imaging study, which protocol
ACR-aligned imaging selection for the clinical scenario, with rationale. Cuts unnecessary studies and surfaces the right one when the obvious choice is wrong.
See ACR layer →When this stops being safe to manage on the floor
Vital sign thresholds, lab trigger values, and clinical findings that mean ICU, RRT, or specialty consult — surfaced from current vitals and labs in the record, not generic textbook bullets.
See it in real workflow →Which specialist to call — and why
Specialist routing with the structured clinical reason embedded. Cuts the 'why are you calling' phase out of the consult and shortens length of stay on the floor.
Learn more →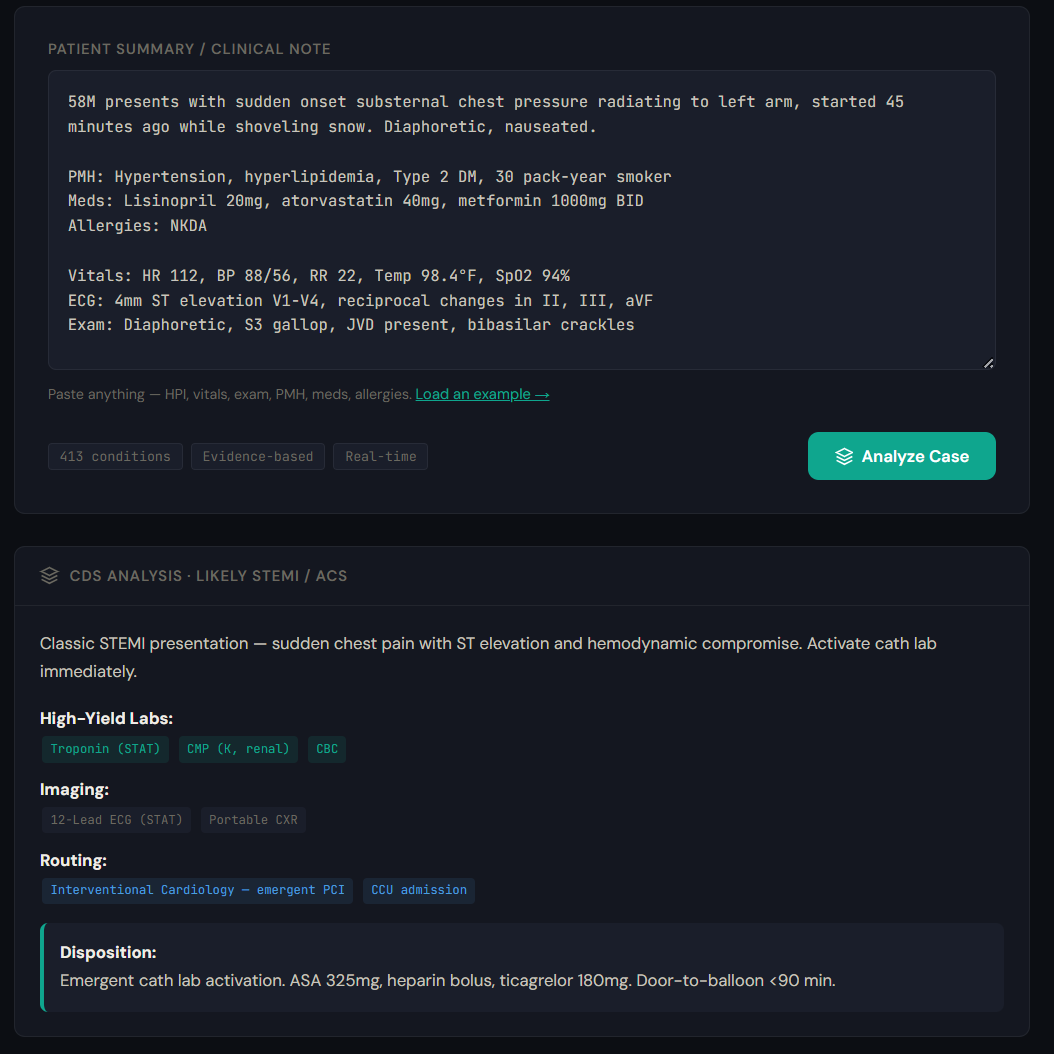
From a free-text note to a structured, traceable decision. STEMI activation, high-yield labs, imaging, specialist routing, and disposition — generated in <200ms. Try it at pogosh.com.
Why Pogosh, not the legacy CDS vendor
Hospitals already pay heavily for clinical decision support. Most of it is static reference content licensed per seat — built for compliance, not for the bedside.
API-native, sub-200ms
Real-time at the point of care. Embed in your EMR, your order set, or your custom workflow. Not a pop-up the clinician dismisses without reading.
Specialty-tailored
413 conditions across 40+ specialties — covered the way the specialty actually thinks about each presentation, not as generic 'chest pain' bullets.
Structured + traceable
Every recommendation maps to a guideline. No hallucinated logic, no LLM-only generation. Clinicians can verify why each suggestion is on screen.
Pricing Founding pricing
Priced per location, unlimited users and API calls. No per-call fees, no throttling. Pogosh is designed as a copilot — called every time a provider opens a chart — so usage-based pricing would create perverse incentives to use it less.
💡 Pay yearly, get 2 months free — switch to annual any time.
per physical location, billed monthly
- Up to 5 providers
- All 413 conditions
- All 40+ specialties
- High-yield lab guidance
- Imaging recommendations
- Specialist routing rules
- Escalation triggers
- Missing order alerts
- OpenEMR module included
- Email support
~$30/provider/month at 5 providers
Start Clinic — $149/mo30-day money-back guarantee. Cancel anytime.
per physical location, billed monthly
- Up to 15 providers
- Everything in Clinic
- Priority support + Slack channel
- Usage analytics dashboard
- Early access to new conditions
- BAA available
~$20/provider/month at 15 providers
Start Practice — $299/mo30-day money-back guarantee. Cancel anytime.
Negotiated annually
- Unlimited providers
- Custom EMR integration
- Dedicated account support
- Custom SLA
- Multi-site licensing
- Bulk condition additions on request
- BAA available
All paid tiers include the full condition library. Pricing is per physical location.
Current tiers are founding pricing. Early customers keep their rate — future price increases never apply to active subscriptions.
The API in 30 seconds
Every tier ships with the same REST API. Base URL: https://api.pogosh.com
curl https://api.pogosh.com/v1/conditions \
-H "Authorization: Bearer YOUR_KEY"GET /v1/conditions— the full condition library, indexed by specialtyGET /v1/condition/:id— structured decision content for a single conditionPOST /v1/evaluate— condition ID + clinical parameters in; labs, imaging, routing, and escalation criteria out
Full API docs → pogosh.com/api
Demo keys (50 req/day) available immediately. Paid keys provisioned same-day after intake review.
Who deploys Pogosh
Pogosh is API-first — the integrations look different by use case.
EHR-embedded clinical intelligence
Hospitalist, EM, and inpatient teams. Pogosh embeds in your EMR via REST API or the OpenEMR module — at the point of order entry or chart open.
Specialty-tailored decision support
IR, urgent care, anesthesia, and specialty teams. Pogosh's specialty layer covers the conditions and decision points that generic CDS misses.
Add guideline-based logic to your platform
EHR vendors, clinical platform companies, and health-tech startups embedding decision logic. Pogosh ships as a backend API — your UX stays yours.
Standardized clinical floor across providers and sites
Locum agencies and telehealth groups whose clinicians rotate through unfamiliar systems. Pogosh provides the institutional context the system itself can't.
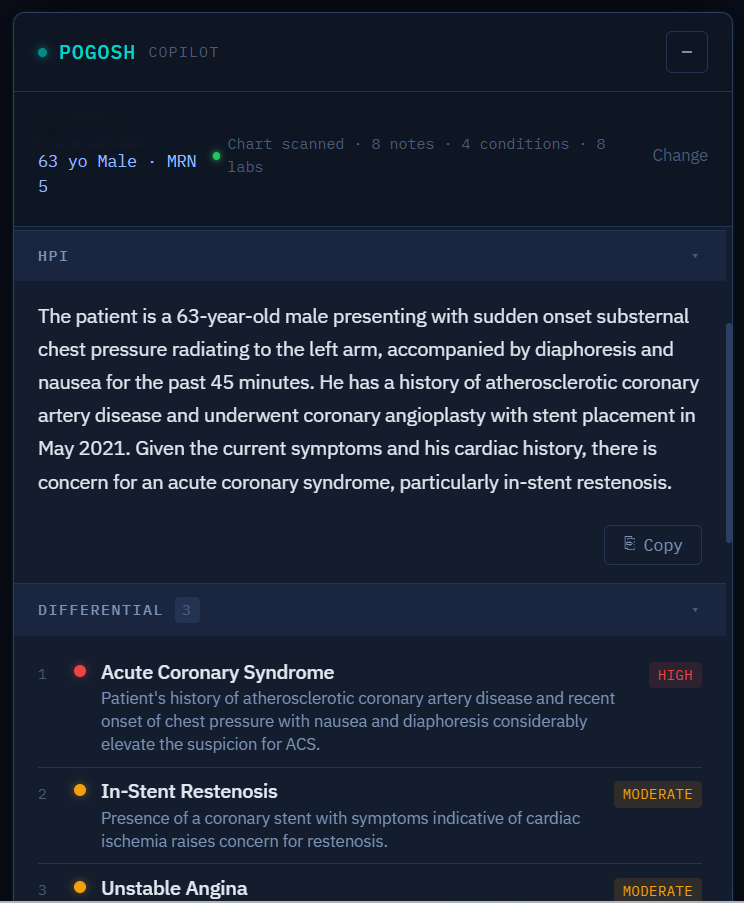
Chart-aware differential, inline. Pogosh CoPilot scans the encounter, conditions, and labs in the open chart — then surfaces a ranked differential with severity tier.
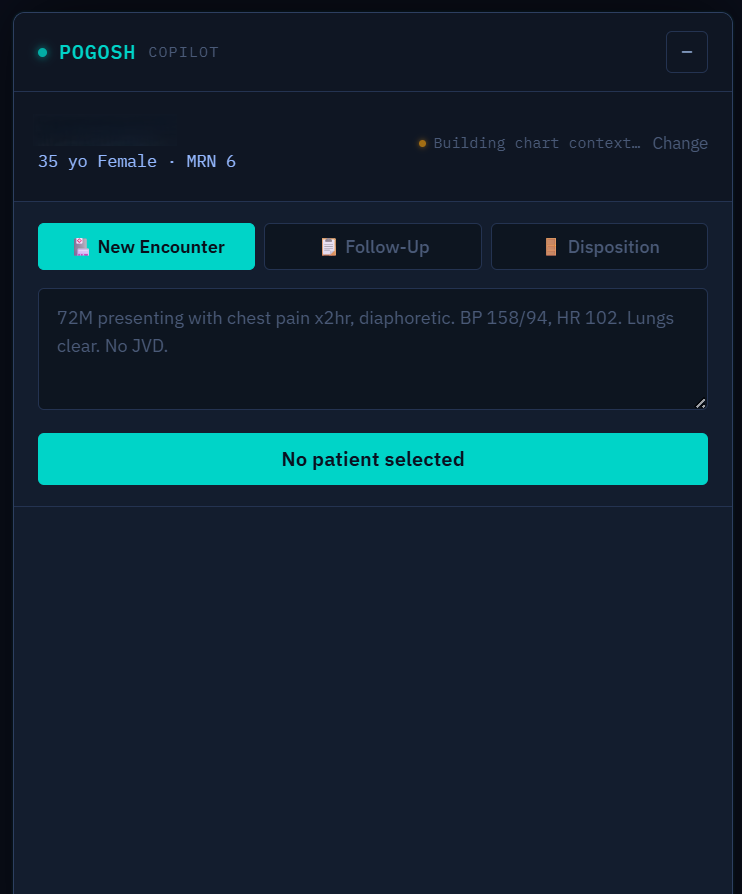
Same engine, three note modes. New encounter, follow-up, and disposition notes — plain-language input, structured note out, grounded in the same chart context.
Three ways in
Pricing is public and self-serve. Start on a tier, try the engine live first, or apply for the validation program.
💳 Start now
Pick a tier and deploy. Clinic from $149/month per physical location — unlimited users and API calls, full condition library, OpenEMR module included.
See pricing →🧪 Try it live
Paste a clinical scenario and watch the structured output — differential, high-yield labs, imaging, specialist routing, and disposition — in real time.
pogosh.com/try →🩺 Clinical Validation Partner
Three months of full Pogosh access at no cost in exchange for structured feedback. We're selecting a small number of clinical sites for real-workflow validation. Validation Partners convert at founding pricing at the end of the 3-month term — locked for the life of the subscription. Free access doesn't linger; the feedback window is the deal.
Apply →Privacy by architecture: Pogosh accepts condition IDs and clinical parameters — not patient identifiers. Security & Data Handling →
Common questions
Is Pogosh an LLM-based tool?
No. Pogosh is a structured rule engine — every recommendation maps to a specific clinical guideline and rationale. It does not generate free-text clinical content. Clinicians can verify the source of every suggestion.
Does Pogosh handle PHI?
Pogosh accepts condition IDs and clinical parameters — not patient identifiers. The integration architecture is designed so PHI doesn't need to leave your system to get the recommendation back.
How does Pogosh integrate with my EMR?
REST API + OpenEMR module. Most hospitals deploy via the API — embedding the response in order entry, chart open, or specialty handoff workflows. Talk to us about your specific EMR.
How does pricing work?
Clinic is $149/month for up to 5 providers, Practice is $299/month for up to 15, and Enterprise — unlimited providers, custom EMR integration, SLA, multi-site — is negotiated annually. Annual billing gets you 2 months free, and every paid tier includes the full condition library. Priced per location, unlimited users and API calls. No per-call fees, no throttling. Pogosh is designed as a copilot — called every time a provider opens a chart — so usage-based pricing would create perverse incentives to use it less.
What specialties are covered?
413 conditions across 40+ specialties — heaviest depth in IR, hospital medicine, EM, anesthesia, vascular surgery, GI, cardiology, and pulmonary. New conditions are added on request when a Validation Partner has a structured need.
Who built it?
Pouyan Golshani, MD — a practicing interventional radiologist — and the GigHz clinical team. Built because no API-native CDS engine existed that surfaced specialty-level decisions in real time.
Make institutional knowledge available on every shift.
Try the live demo, then pick a tier — Clinic from $149/month per physical location, unlimited users and API calls. 30-day money-back guarantee.
Pogosh CDS surfaces guideline-based recommendations to support clinical decision-making. It does not replace clinician judgment, and every recommendation should be evaluated by the clinician at the point of care. A GigHz product. Built by Pouyan Golshani, MD.
Written and reviewed by Pouyan Golshani, MD, Interventional Radiologist — Last updated May 26, 2026
Part of the GigHz library: systems doctors were never taught.